
The growth of New York’s Medicaid spending is projected to slow but not stop as Governor Hochul and the Legislature effectively split their differences over health care in the newly enacted state budget.
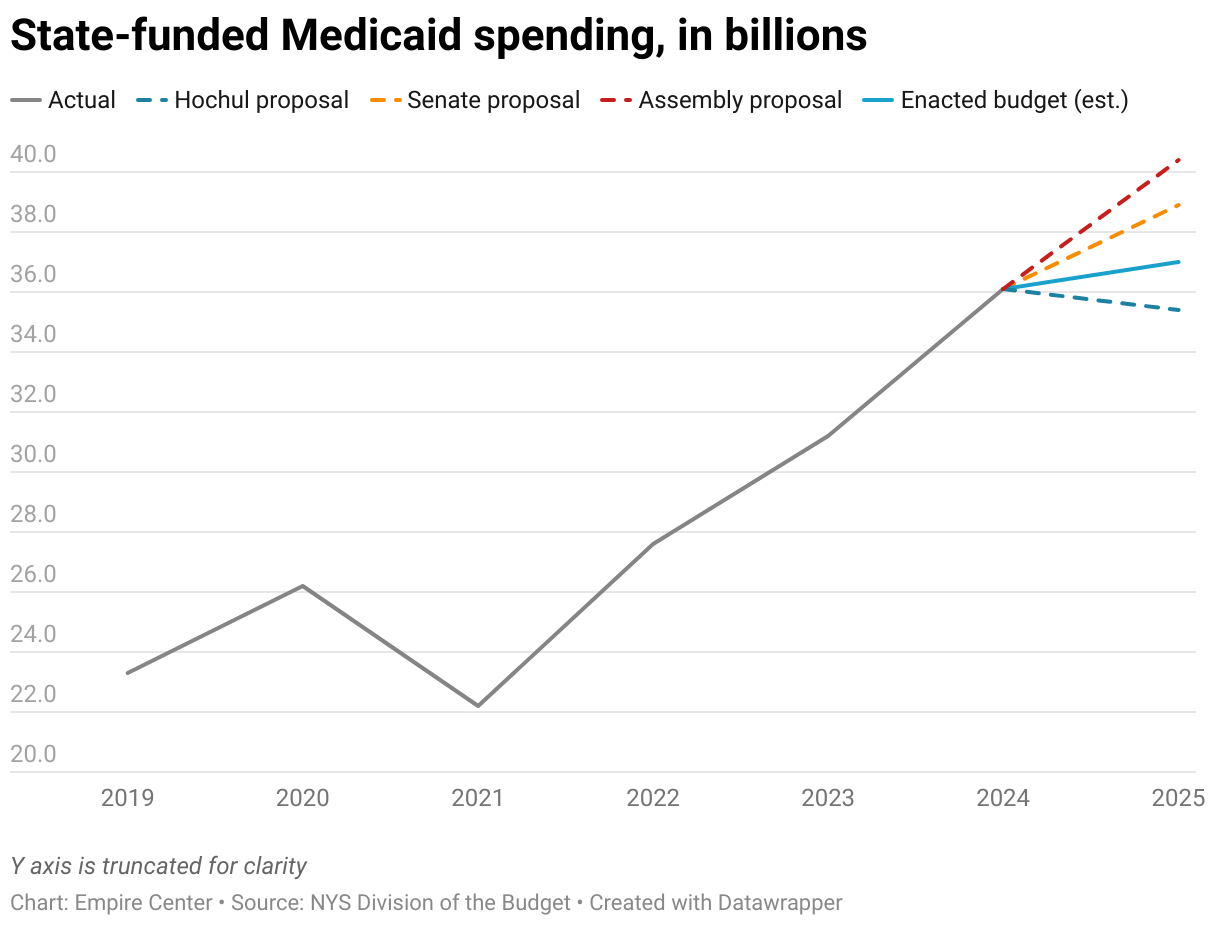
Total state funding for Medicaid in fiscal 2025 will be $37 billion, up $900 million or 3 percent from the year before, according to a preliminary estimate from the governor’s office.
That would be the smallest increase of Hochul’s tenure, during which the state share of Medicaid jumped 13 percent in 2023 and 15 percent in 2024.
The final state-share amount falls roughly in the middle between Hochul’s initial spending plan and the counter-proposals from the Legislature (see chart). Hochul had proposed to reduce the state share by about 2 percent while the Senate and Assembly called for increases of 8 percent and 12 percent, respectively.
An official estimate of total Medicaid spending is not yet available, but it’s likely to approach $113 billion, including $67 billion in federal aid and $9 billion in mandated contributions from New York City and the 57 other counties.
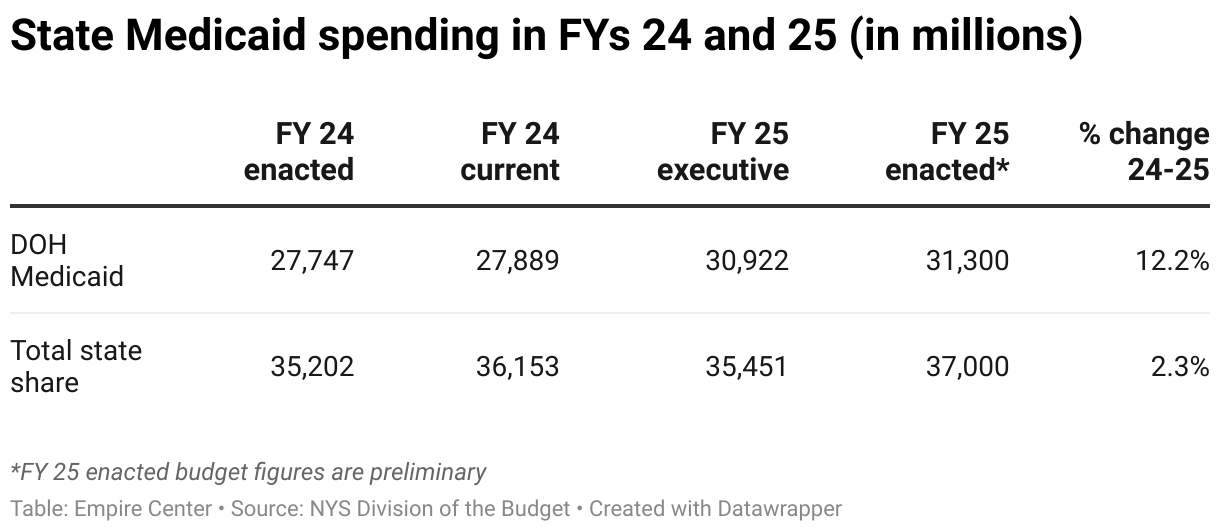
It should be noted that Medicaid has repeatedly overrun its expected spending in recent years. In fiscal 2024, the state share of Medicaid spending exceeded its initially budgeted amount by almost $1 billion (see table).
Setting the stage for future growth, the budget levied a new tax on health insurance plans, which are also known as managed care organizations, or MCOs. Supporters have portrayed the MCO tax as a way of generating $4 billion in additional Medicaid funding without significantly affecting commercial insurers and their customers – similar to how a recently enacted MCO tax is working in California.
However, it’s not clear that other states will receive federal approval for a California-style tax. Also, the authorizing language for New York’s tax delegates the details to the health commissioner, giving him broad latitude to depart from the California model.
Revenue from the tax will flow to a newly created Healthcare Stabilization Fund, where it will be available to either increase or replace state funding for Medicaid. Although it’s unclear how much revenue the levy will generate – or when it will take effect – the budget includes an initial appropriation of $350 million from the stabilization fund.
New spending in the budget includes Medicaid rate increases worth $525 million a year for hospitals and $285 million a year for nursing homes and assisted living facilities. This represents at least a partial victory for the two industries’ multi-million-dollar ad campaigns pushing for higher Medicaid compensation.
The budget authorized the increases as lump sums rather than an across-the-board percentage increases, allowing Health Department officials discretion to give some facilities larger bumps than others.
Another major provision in the budget overhauls the Consumer Directed Personal Assistance Program, in which people with disabilities can hire friends and family members to be their in-home caregivers, with Medicaid paying their wages. The program’s enrollment and costs have grown explosively in recent years, and Hochul had proposed eliminating wage supplements for caregivers as a way of saving money.
Instead, she and Legislature agreed to eliminate most of the hundreds of middle-man companies, known as “fiscal intermediaries,” that have sprung up in the past decade to handle payroll processing for the program. As of January, the state will contract with a single fiscal intermediary for the entire state – and that company will subcontract with a dozen or two long-term fiscal intermediaries, all or most of which are not-for-profit organizations serving the disabled.
Officials estimate the consolidation will save Medicaid about $500 million, including $200 million in state funds.
This proposal, which emerged late in budget talks, was supported by the health-care union 1199 SEIU. Some observers believe that establishing a single, statewide fiscal intermediary could pave the way for 1199 to unionize the thousands of caregivers who are paid through the program – as has happened in other states.
At Hochul’s behest, the budget also establishes a “safety-net transformation program,” with the stated goal of improving the quality and financial stability of safety-net hospitals.
Effectively, this program is retroactively putting additional strings on $2.6 billion that was allocated for health-care capital grants in the two previous budgets, nearly all of which remains unused. Those grants will now be limited to safety-net hospitals that develop a turnaround plan in conjunction with a “partner organization,” which is loosely defined to include “health systems, hospitals, health plans, residential health care facilities, physician groups, community-based organizations or other health care entities.”
The budget also allocated $300 million in operating funds for this program, and authorizes the health commission to waive certain regulations “to allow applicants to more effectively or efficiently implement projects.”
However, it’s hard to know how much difference that will make because the program rules out waivers pertaining to:
[P]atient safety, patient autonomy, patient privacy, patient rights, quality of care, safe staffing, adverse event reporting, due process, scope of practice, professional licensure, environmental protections, infection control, provider reimbursement methodologies, character and competence, or occupational standards and employee rights.
About the Author

You may also like

The Attorney General’s MFCU SNAFU
Attorney General Letitia James' latest fight with the Trump administration focuses on New York's Medicaid Fraud Control Unit, a federally funded agency housed in James' office.
On T Read More

Healthcare Revelations in the Enacted Budget Financial Plan
The state financial plan published on June 10 disclosed key information about healthcare revenue and spending that lawmakers had not made public when approving the annual budget two weeks before.
Read More

Federal Suit Traces Medicaid Fraud to the Top of NYS Government
The Trump administration's latest salvo against Medicaid fraud takes aim at a different kind of target – two high-ranking New York officials along with a major state contractor.
A Read More

Healthcare Highlights in the New State Budget
Governor Hochul's focus on affordability seems to have skipped over the healthcare portions of the new state budget.
The deal finalized May 27 Read More

Lawmakers Consider Hiking Fees for Filling Prescriptions
UPDATE: The proposal discussed below passed the Assembly Friday evening by an unofficial vote of 133-0. Having previously been approved by the Senate, the bill will head to Governor Hochul's desk for her signature or ve Read More

Budget Deal Reportedly Earmarks $100M for 1199 and Extends MCO Tax
As Governor Hochul and legislative leaders rush to finalize the overdue state budget, outlines of some healthcare-related deals have begun to emerge from the closed-door negotiations.
Read More

Four Problems with a Statewide Pied-à-Terre Tax
Soon after Governor Hochul floated the idea of a "pied-à-terre" tax in New York City, Albany Sen. Patricia Fahy proposed to expand the concept to the rest of the state.
As with H Read More

Albany Should Listen to Jamie Dimon
In his annual message to shareholders, JP Morgan Chase's chief executive, Jamie Dimon, offered a timely and pointed warning for New York policymakers.
It's worth , with emphasis add Read More